Health Insurance Programs Documents
Health Insurance Programs
Cigna Claim Form Instructions and Details
This document provides instructions for filling out the Cigna Claim Form, including necessary information, payment options, and other coverage details.
Health Insurance Programs
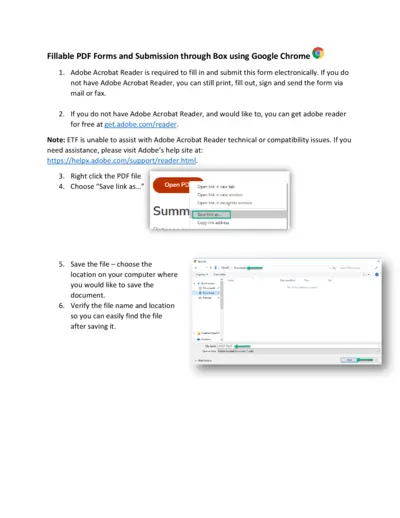
Health Insurance Application for Wisconsin Employees
This PDF form allows Wisconsin employees to apply for health insurance coverage or make changes. It includes instructions for filling out the form and submitting it electronically through Box. Ensure all information is accurate for timely processing.
Health Insurance Programs
Institute for Advanced Study Health Insurance Subsidy
This application form is for members of the Institute for Advanced Study seeking health insurance subsidies. Complete and return it to the Human Resources department. Ensure all eligibility criteria are met before submission.
Health Insurance Programs
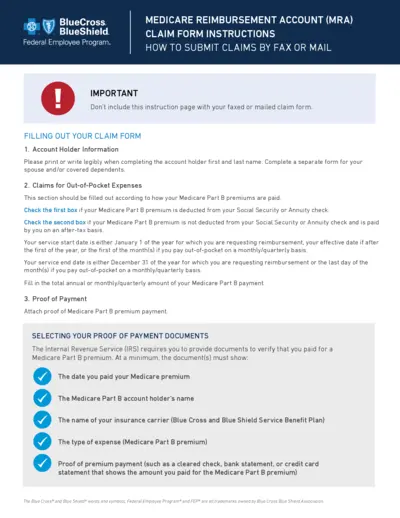
Medicare Reimbursement Account Claim Form Instructions
This file provides detailed instructions on filling out the Medicare Reimbursement Account Claim Form. It guides users on how to submit claims for out-of-pocket Medicare expenses. Ideal for individuals seeking reimbursement for their Medicare Part B premiums.

Health Insurance Programs
Request to Cancel Health Insurance Policy
This file is a request form to cancel your health insurance policy with Arkansas Blue Cross and Blue Shield. It outlines the necessary fields to complete and the process to follow for cancellation. Ensure all information is accurately provided for a smooth cancellation experience.

Health Insurance Programs
AARP Medicare Advantage Enrollment Request Form
The AARP Medicare Advantage Enrollment Request Form is designed for individuals looking to enroll in a Medicare Advantage plan provided by UnitedHealthcare. This form collects essential information for processing your enrollment. Fill it out accurately to ensure a smooth enrollment experience.

Health Insurance Programs
Health and Dental Enrollment Form Instructions
This enrollment form allows individuals to apply for group health and dental coverage. It's designed for employees to provide necessary personal information, dependent details, and coverage choices. Follow the instructions carefully to ensure proper submission.
Health Insurance Programs
Request for Cashless Hospitalisation Health Insurance
This file is a request form for cashless hospitalization under STAR Health Insurance. It includes detailed patient information, treatment specifics, and necessary documentation. Use this form to streamline your health insurance claims process.
Health Insurance Programs
New York State Health Insurance Claim Form Instructions
The New York State Health Insurance Claim Form is essential for submitting claims for medical services. This PDF provides crucial guidelines for completing and submitting your claim efficiently. Follow the instructions within to ensure prompt processing of your claims.
Health Insurance Programs
BlueCross BlueShield NC Member Appeal Form Instructions
This Member Appeal Form is essential for BlueCross BlueShield of North Carolina members seeking to file an appeal. It includes detailed instructions on how to complete and submit the form. Follow the guidelines to ensure a successful appeal process.
Health Insurance Programs
Regence Blue Cross Blue Shield Enrollment Form
This form is a crucial document for enrollment and changes in health insurance through Regence Blue Cross Blue Shield of Oregon. It includes instructions for completing the application and details about coverage options. Ensure all information is accurate to avoid delays in processing your application.
Health Insurance Programs
EmblemHealth Complaint Appeal Instructions
This file provides important information on how to file a complaint appeal with EmblemHealth. It outlines the rights you have regarding complaint appeals and how to properly submit your appeal. Clear instructions and contact details are included for your convenience.